🩺 SECOND-DEGREE ATRIOVENTRICULAR (AV) BLOCK – DIAGNOSIS AND MANAGEMENT GUIDE
Author: Doctor Chu – Specialist in Functional Diagnostics, with expertise in Electrocardiography (ECG)
🔹 1. Overview
Atrioventricular (AV) block is a conduction disturbance in which the electrical impulses from the atria fail to reach the ventricles properly.
In second-degree AV block, some atrial impulses are not conducted through the AV node, resulting in P waves that are not followed by QRS complexes.
This condition may be transient or progressive and is considered a warning sign for complete (third-degree) AV block, a potentially life-threatening cardiac emergency.
🔹 2. Pathophysiology
Common causes include:
-
Structural heart disease: Myocardial infarction (especially inferior or anterior wall).
-
Degeneration of the conduction system (Lenègre’s or Lev’s disease).
-
Medications: Digitalis, beta-blockers, calcium channel blockers (verapamil, diltiazem), amiodarone.
-
Functional causes: Increased vagal tone, electrolyte disturbances (notably K⁺, Mg²⁺).
-
Post-cardiac surgery, myocarditis, or systemic diseases (sarcoidosis, amyloidosis).
🔹 3. Clinical Manifestations
Symptoms depend on the degree of block and the ventricular rate:
-
May be asymptomatic if transient.
-
Dizziness, fatigue, palpitations, especially with a low ventricular rate.
-
Syncope or Adams–Stokes attacks if conduction pauses are prolonged.
-
Bradycardia and irregular pulse may be detected by auscultation or palpation.
Physical examination findings:
-
Irregular pulse with occasional dropped beats.
-
Variable intensity of the first heart sound (S1); “dropped beats” may be heard.
🔹 4. Electrocardiographic Diagnosis (ECG)
Second-degree AV block is diagnosed when:
Some P waves are not followed by QRS complexes, while others are normally conducted.
There are two main types and a severe variant:
🧩 4.1. Mobitz Type I (Wenckebach Phenomenon)
-
Progressive lengthening of the PR interval until a P wave fails to conduct (no QRS).
-
The pattern then repeats cyclically.
-
QRS complexes are usually narrow, indicating a lesion at the AV node.
-
Often benign, commonly seen in athletes or young, healthy individuals.
🧩 4.2. Mobitz Type II
-
PR intervals remain constant, but occasionally a P wave is not conducted (missing QRS).
-
QRS complexes are often wide, suggesting a lesion below the AV node (His bundle or bundle branches).
-
More dangerous, with a higher risk of progression to complete heart block.
-
Requires close monitoring and early intervention.
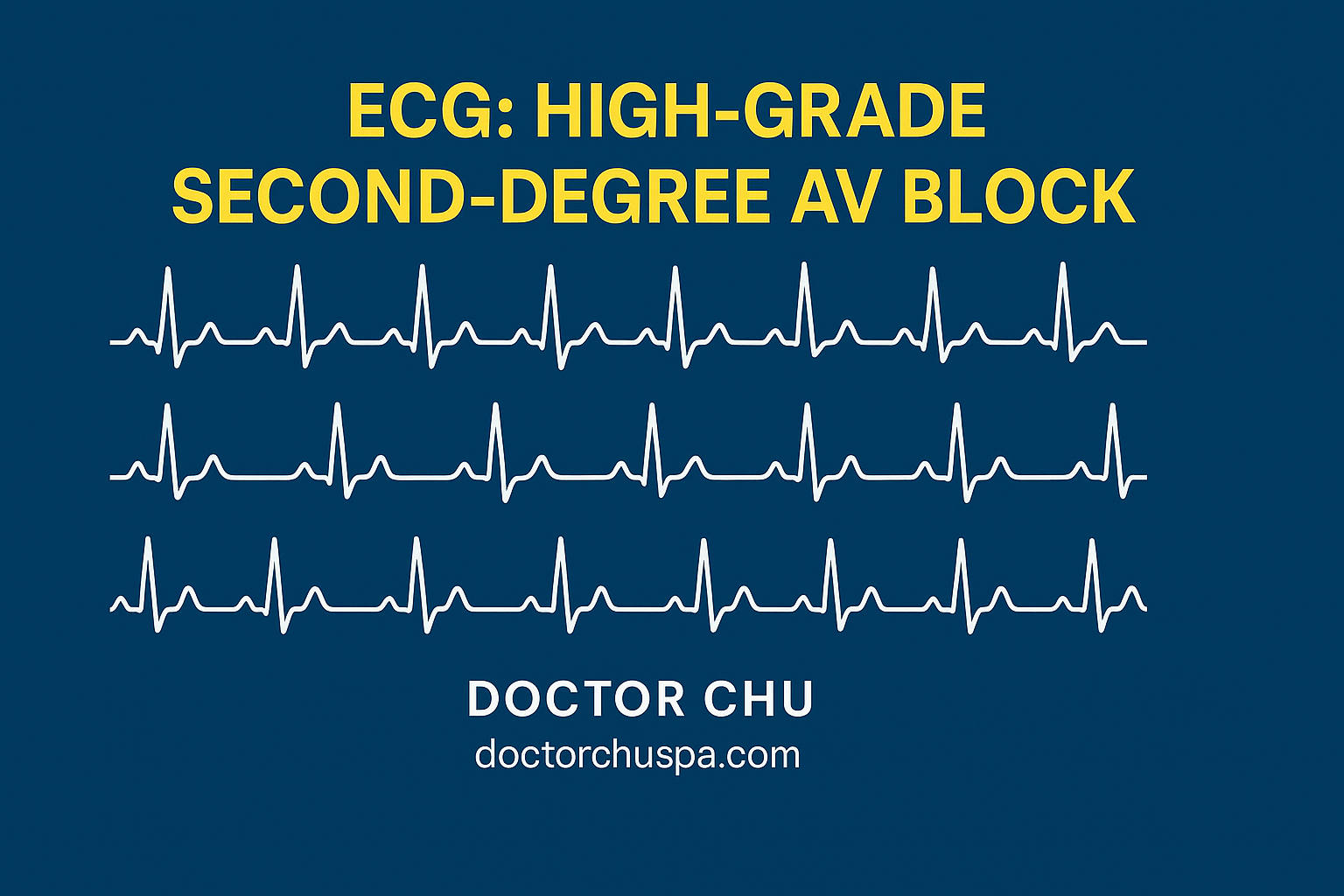
🧩 4.3. High-grade Second-degree AV Block
-
Only one of every three or four P waves is conducted (3:1 or 4:1 ratio).
-
Ventricular rate is very slow (30–40 bpm).
-
Considered a severe form, often a precursor to complete block.
-
Emergency pacemaker insertion is typically indicated.
🔹 5. Management and Treatment
🏥 5.1. General Principles
-
Assess symptoms and ventricular rate.
-
Identify and eliminate reversible causes (medications, electrolyte imbalance, ischemia).
-
Continuous ECG monitoring is essential.
💊 5.2. Specific Treatment
👉 Mobitz Type I (Wenckebach)
-
Asymptomatic: Observation; no specific therapy required.
-
Symptomatic (syncope, fatigue):
-
Atropine 0.5 mg IV, repeat every 3–5 minutes (maximum 3 mg).
-
If unresponsive → dopamine or epinephrine infusion at low doses.
-
Temporary pacing may be considered for persistent bradycardia.
-
👉 Mobitz Type II or High-grade AV Block
-
High risk of progression to complete block.
-
Immediate temporary pacing is indicated, especially if:
-
Ventricular rate < 40 bpm.
-
Presence of syncope, hypotension, or altered mental status.
-
-
Permanent pacemaker implantation should follow if the block does not resolve within 7–10 days.
⚡ 5.3. Treat Underlying Causes
-
Discontinue AV nodal blocking drugs (digitalis, beta-blockers, calcium channel blockers).
-
Correct electrolyte imbalances.
-
Manage underlying conditions: myocarditis, myocardial infarction, endocrine disorders, or toxicity.
🔹 6. Long-term Follow-up
-
Regular check-ups with a cardiologist.
-
Pacemaker monitoring (if implanted).
-
Periodic ECG or 24-hour Holter monitoring to evaluate rhythm stability.
-
Avoid medications affecting AV conduction without medical supervision.
🔹 7. Summary Table
| Type of Block | Site of Lesion | QRS | Prognosis | Management |
|---|---|---|---|---|
| Mobitz I | AV node | Narrow | Good | Observation; atropine if symptomatic |
| Mobitz II | Below AV node (His or bundle branch) | Wide | Poor | Temporary or permanent pacemaker |
| High-grade | Infranodal, widespread | Wide | Very poor | Emergency pacing required |
🔹 8. Conclusion
Second-degree AV block is a significant warning sign in the cardiac conduction system.
Early recognition and timely management can prevent progression to complete heart block and reduce the risk of sudden cardiac death.
“A correctly interpreted ECG at the right moment can save a life.” – Doctor Chu
🌐 Further Learning & Contact Information
Course: Practical ECG Interpretation – From Basic to Advanced
📍 Website: doctorchuspa.com
📺 YouTube: Doctor Chu – The Doctor for the Poor
📱 TikTok: Doctor Chu – The Doctor for the Poor
